

“We would wish to share with you the following remarks. Our Comboni Family (MCCJ-CLM-CMS-SCM) has a long and valuable tradition of engagement in various pastoral activities with a strong social dimension. We also have a well-established history of 12 years of participation in the World Social Forum and the Comboni Forum “
“… In the 2018 Comboni Forum, held in Salvador de Bahia (Brazil) on the occasion of the World Social Forum, the participants suggested that all members of the Comboni Family engaged in social ministry could reflect on their activities. To look at this ministry from the light of the Gospel and of our specific Charism, the participants proposed an analysis and evaluation all the activities in which we are engaged. At our recent meeting of the two General Councils in April 2019 and of the General Administrations of the four branches of the Comboni Family in June 2019, we welcomed this proposal and we decided to create a commission that could draw up a roadmap and coordinate the various activities to implement the proposal… “
The nominated commission consists of:
Daniele Moschetti, (danielemoschetti15@gmail.com), mccj
Sr. Hélèn Israel Soloumta Kamkol (isralvi@yahoo.fr), smc
Marco Piccione (Venegono): (marcopiccione78@gmail.com), lmc
Sr. Maria Teresa Ratti (mtratticms@gmail.com), smc
Fernando Zolli (combonifi@gmail.com), mccj
What is reported is an extract from the letter with which the general superior of the MCCJ (P. Tesfaye Tadesse) and the general superior of the Comboni Sisters (Sr. Luigia Coccia) communicated at the same time the birth of the commission for the ministry and the purposes of this commission.
Over the months, some people have added to the commission who have made an indispensable contribution in terms of experience and knowledge in order to achieve the most complete and exhaustive possible work.
The three concrete activities that the commission had undertaken to achieve its objectives are:
- Map all the social ministerial activities of the Comboni Family
- Publish the 2nd volume, which follows the 1st from the title: “Be the change you want to see in the world”
- Organize participation in the World Social Forum (FSM) 2020
For the first activity many of you have already been involved and we take this opportunity to thank you for your valuable contribution. From the collection of all the files received by the commission, a database will be drawn up thanks to which it will be possible to have a photograph of all the social and JPIC activities in which the Comboni family is engaged in the world.
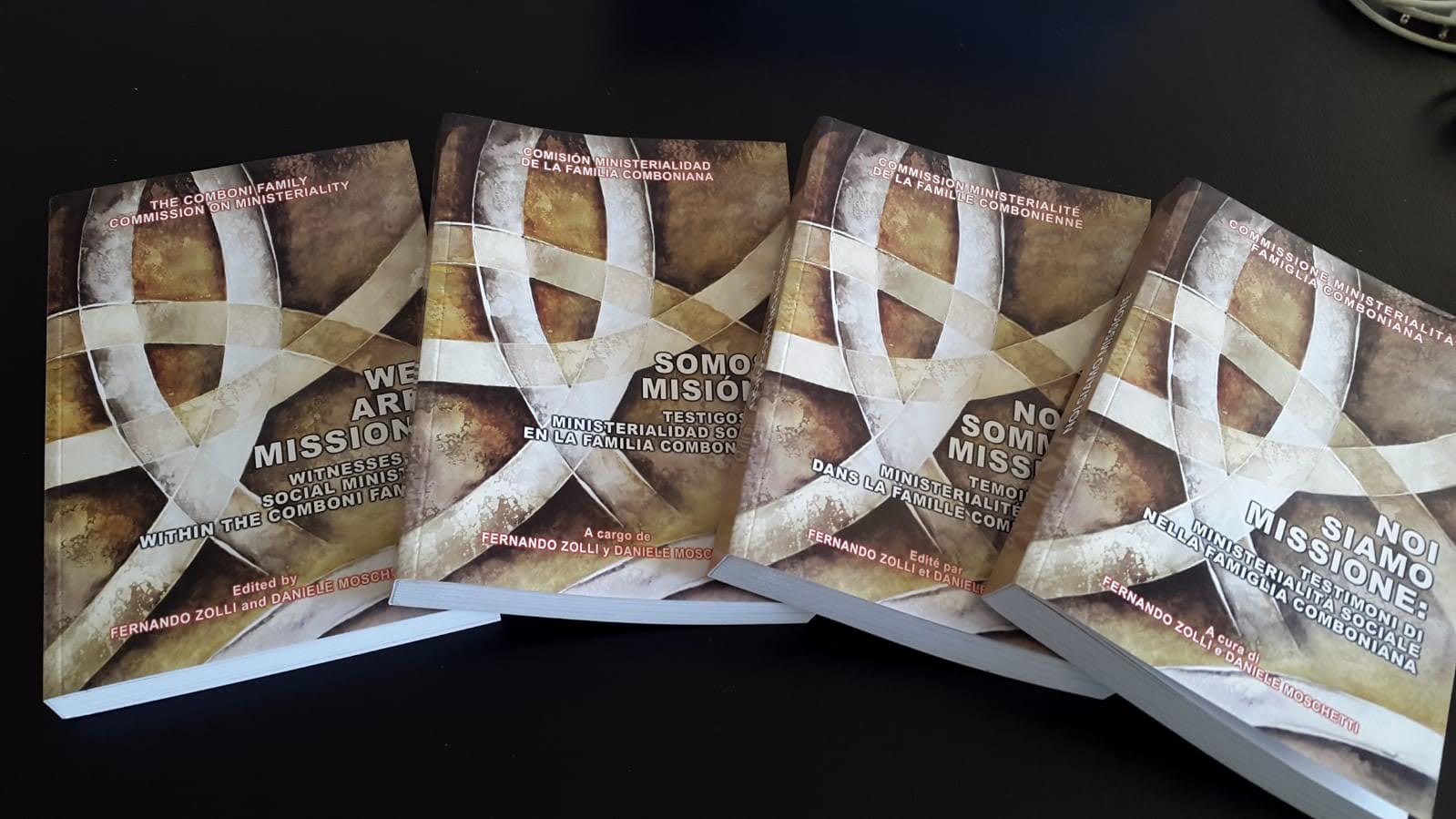
But this post wants, above all, to give you the good news that has been completed and that is now available, the 2nd volume of the book on social ministry of the Comboni family entitled “WE ARE MISSION: witnesses of social ministry in the Comboni family“, which presents with more detailed informations, some projects in which fathers, brothers, sisters, seculars or lay people are engaged and which have been considered particularly significant to illustrate the methods and style to live the aspect of the Comboni charism which provides for a concrete social commitment. Alongside the presentation of these projects, there are some reflections from witnesses who will certainly be able to help in reflection and discernment on these issues that are so important and, I would say, characterizing our being Combonians.
The book is available in four languages (Italian, English, French and Spanish). It will be distributed in the Comboni houses but some copies will be reserved for the laity.
Unfortunately, the last activity foreseen for the commission, namely the participation in the WSF initially scheduled for 2020, is currently pending. In fact, due to the sad health situation that is affecting the whole world, the forum has been postponed to 2021.
Instead, the forum of the Comboni family usually scheduled immediately after the WSF, it was decided to do it in another period. At this time, it has been set from 12 to 16 December 2020.
Hoping that the tool of the book will help us in our daily mission and in feeling even more family united by the gift we have received of the Comboni charism, we greet you and send you our best wishes and prayers so that even from this difficult moment we can get out more fortified in faith and in the certainty of being accompanied by a God who walks with us.
Marco Piccione, CLM